Community dialogues to support maternal health: lessons from the world’s newest nation
By Sally Theobald, 26 November 2014
We have recently been in Hawassa, Southern Ethiopia. The visit was brilliantly hosted by our REACHOUT partner REACH Ethiopia.
Two of our colleagues, Korrie de Koning from the Royal Tropical Institute (KIT), The Netherlands and Kingsley Chikaphupha from REACH Trust Malawi, came straight to Hawassa from South Sudan, where they have been working on the community participation component of the ‘SHARP’ programme in northern Bahr el Ghalzal.
The SHARP programme is funded by the Dutch Government and is a collaboration of the South Sudanese Ministry of Health, the Royal Tropical Institute, IMC, Healthnet TPO and Cordaid. Community engagement is an area of action in our REACHOUT Quality Improvement Cycles which aim to improve close to community services.
As part of our capacity development activities Korrie and Kingsley shared their experiences on community engagement in maternal health in the world’s newest country, South Sudan.
The context
At 2,054 maternal deaths per 100,000 live births South Sudan has the highest maternal mortality in the world.
At marriage, women’s families are paid a bride price, which in Northern Bahr el Ghazal (NBeG), is paid in cows. Girls are seen as an investment and looked after well until they are married off - often in early adolescence. South Sudan is in transition. With years of conflict and the construction of a new nation, existing gender norms which expect women to bear many children have been intensified in order ‘to replace the ones that were lost’. Gender and societal norms are also in transition. Elders complain that the young no longer listen to and respect their elders, couples do not keep to the traditional three years birth spacing, and marry younger and younger. Parents worry that their girl may get pregnant before marriage so they marry her off early, especially if she is not in school. Girls and boys have very limited access to sex education or contraceptives. These factors can lead to early pregnancy.
Using community dialogue to enable reflection

KIT developed a curriculum for the training of community facilitators to support dialogue and reflection on norms and values shaping maternal mortality and health service access and use. The curriculum was shaped by various sources, but drew substantially on the GTZ developed generational dialogue. The curriculum was further adapted with input from the Community District Health Department in Wau, WBeG and Aweil North in NBeG, REACH Trust, International Medical Corps, and Healthnet TPO. Training of facilitators focussed on dialogue between older and younger women and men, comparing social and gender norms and practices between present and past, sharing knowledge on maternal health and discussing what needs to be changed for maternal health to improve.
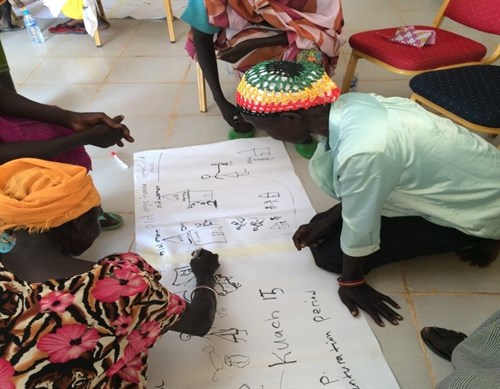
Groups used drawings, statements and proverbs to explore the relationships between communities by gender and generation. For some women, this was their first experience of holding a pen or pencil but they were skilled in drawing images of maternal health decisions, dilemmas and outcomes throughout their life cycle. The ‘but why’ technique was used to probe and understand the rationale behind different cultural norms, their meanings and whether they were seen as fair.
Kingsley facilitated the men’s groups and explained at first there was complete refusal to even entertain the possibility of a discussion on contraception but use of the 'but why' technique enabled discussion on the impact of multiple births on (especially young) women and child survival rates. This led to some shifts in viewpoints. Drama was also used, and women acted out what it is like to have obstetric fistula, and how women with urinary or faecal incontinence were treated within their communities. Following work in women and men only groups, the community fed back their ideas and experiences to each other, and for many women (who are very powerful within their own domains) this was their first experience of speaking publicly in front of men.
Community dialogues and commitments to change
Through the facilitated discussions between genders and generations statements for change were negotiated and agreed. Here are some examples:
- “If a man with more than one wife is not looking after one of his wives and their children, the wife has the possibility to refuse to produce any more children without having to pay back the cows/bride price and also has the right to not be beaten.”
- “We don’t want daughters to marry or be pregnant before 18 years old and we in our family will do all we can – we want to pledge this to our family and community.”
- “Married women should be allowed to use contraception and have three year birth spacing.”
This is an inspiring example of how community engagement can shift gender and societal norms and shows great facilitation skills from Korrie and Kingsley. Facilitators are being trained at local level and the approach will be rolled out and hopefully continue to challenge and change views and practices that undermine women’s maternal health.
Recent news
- A REACHOUT update from Malawi, 25 November 2014
- Reflections on a visit to the Pregnant Women's Forum in Howoleso Kebele, Southern Ethiopia, 21 November 2014
- REACH Ethiopia win the Kochon Award for their services to TB, 29 October 2014

This project is funded by the European Union.